Created
Initial SOAP note created for patient James Thornton following comprehensive examination. Chief complaint, subjective findings, and objective clinical observations documented.
 Jatin Yadav
Jatin YadavCreate a AI-Powered Dental Clinic Operating System as centralized SaaS platform




























Sign in to leave a comment
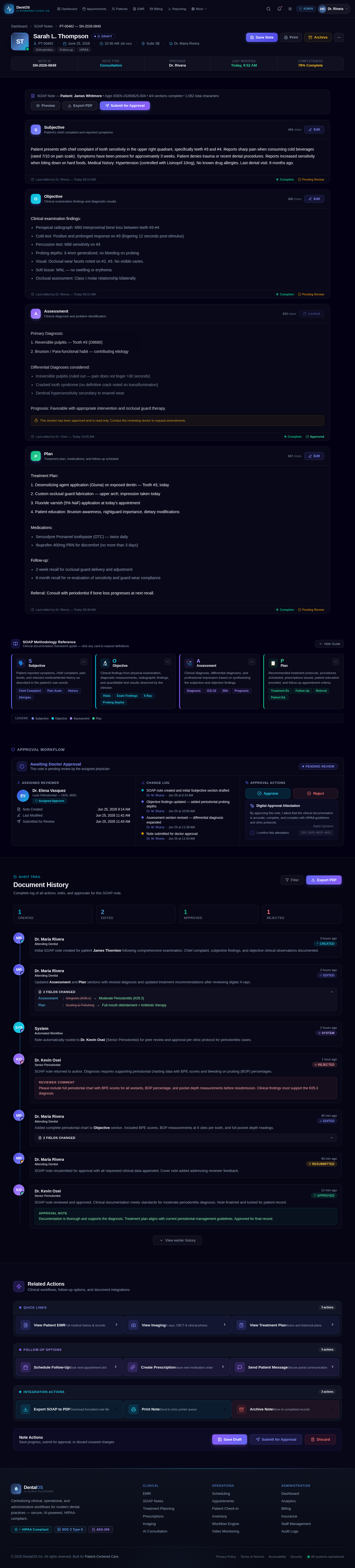
Patient presents with chief complaint of tooth sensitivity in the upper right quadrant, specifically teeth #3 and #4. Reports sharp pain when consuming cold beverages (rated 7/10 on pain scale). Symptoms have been present for approximately 3 weeks. Patient denies trauma or recent dental procedures. Reports increased sensitivity when biting down on hard foods. Medical history: Hypertension (controlled with Lisinopril 10mg), No known drug allergies. Last dental visit: 8 months ago.
Clinical examination findings:
Primary Diagnosis:
1. Reversible pulpitis — Tooth #3 (D8680)
2. Bruxism / Para-functional habit — contributing etiology
Differential Diagnoses considered:
Prognosis: Favorable with appropriate intervention and occlusal guard therapy.
Treatment Plan:
1. Desensitizing agent application (Gluma) on exposed dentin — Tooth #3, today
2. Custom occlusal guard fabrication — upper arch; impression taken today
3. Fluoride varnish (5% NaF) application at today's appointment
4. Patient education: Bruxism awareness, nightguard importance, dietary modifications
Medications:
Follow-up:
Referral: Consult with periodontist if bone loss progresses at next recall.
Patient-reported symptoms, chief complaint, pain levels, and relevant medical/dental history as described in the patient's own words.
The Subjective section captures everything the patient communicates — onset, duration, character, and severity of symptoms. It includes past dental history, medical conditions, current medications, and social factors affecting oral health.
Clinical findings from physical examination, diagnostic measurements, radiographic findings, and quantifiable test results observed by the clinician.
Objective data encompasses direct clinical observations: periodontal probing depths, radiographic bone levels, pulp vitality testing, intraoral photographs, CBCT findings, and any measurable signs present during the appointment.
Clinical diagnosis, differential diagnoses, and professional impression based on synthesizing the subjective and objective findings.
The Assessment represents the clinician's professional judgment — the primary diagnosis (with applicable ICD-10 codes), differential diagnoses considered, prognosis for affected teeth, and the clinical reasoning connecting findings to conclusions.
Recommended treatment protocols, procedures scheduled, prescriptions issued, patient education provided, and follow-up appointment criteria.
The Plan outlines all next steps: immediate procedures (extractions, RCT, scaling), prescriptions with dosing, specialist referrals, home care instructions, and the timeline for re-evaluation. It links directly to the Treatment Planning and Prescriptions modules.
By approving this note, I attest that the clinical documentation is accurate, complete, and complies with HIPAA guidelines and clinic protocols.
Complete log of all actions, edits, and approvals for this SOAP note.
Initial SOAP note created for patient James Thornton following comprehensive examination. Chief complaint, subjective findings, and objective clinical observations documented.
Updated Assessment and Plan sections with revised diagnosis and updated treatment recommendations after reviewing digital X-rays.
Note automatically routed to Dr. Kevin Osei (Senior Periodontist) for peer review and approval per clinic protocol for periodontitis cases.
SOAP note returned to author. Diagnosis requires supporting periodontal charting data with BPE scores and bleeding on probing (BOP) percentages.
Added complete periodontal chart to Objective section. Included BPE scores, BOP measurements at 6 sites per tooth, and full pocket depth readings.
SOAP note resubmitted for approval with all requested clinical data appended. Cover note added addressing reviewer feedback.
SOAP note reviewed and approved. Clinical documentation meets standards for moderate periodontitis diagnosis. Note finalized and locked for patient record.
No comments yet. Be the first!