jolly-doctor
 Jatin Yadav
Jatin YadavI want to create SPA for the attached requirement pdf and color palletes are attached in the image




























Comments (0)
Sign in to leave a comment
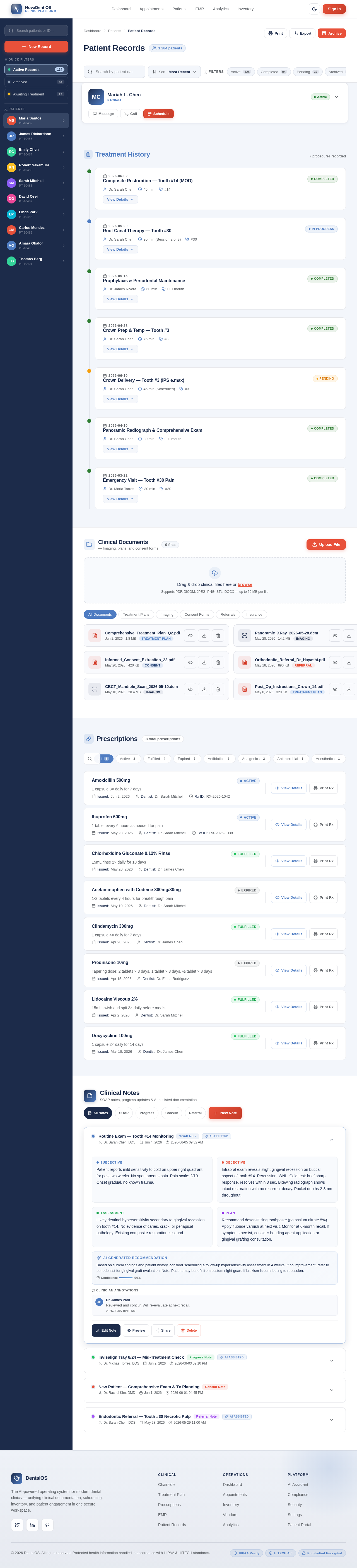
Patient Records
1,284 patientsTreatment History
7 procedures recordedComposite Restoration — Tooth #14 (MOD)
Root Canal Therapy — Tooth #30
Prophylaxis & Periodontal Maintenance
Crown Prep & Temp — Tooth #3
Crown Delivery — Tooth #3 (IPS e.max)
Panoramic Radiograph & Comprehensive Exam
Emergency Visit — Tooth #30 Pain
Clinical Documents
— Imaging, plans, and consent formsDrag & drop clinical files here or browse
Supports PDF, DICOM, JPEG, PNG, STL, DOCX — up to 50 MB per file
Comprehensive_Treatment_Plan_Q2.pdf
Panoramic_XRay_2026-05-28.dcm
Pre_Op_Photos_Set_2026-05-25.jpg
Informed_Consent_Extraction_22.pdf
Orthodontic_Referral_Dr_Hayashi.pdf
Insurance_PreAuth_Molar_RCT.pdf
CBCT_Mandible_Scan_2026-05-10.dcm
Post_Op_Instructions_Crown_14.pdf
Intraoral_Scan_STL_Upper.stl
Prescriptions
8 total prescriptionsAmoxicillin 500mg
Active1 capsule 3× daily for 7 days
Ibuprofen 600mg
Active1 tablet every 6 hours as needed for pain
Chlorhexidine Gluconate 0.12% Rinse
Fulfilled15mL rinse 2× daily for 10 days
Acetaminophen with Codeine 300mg/30mg
Expired1-2 tablets every 4 hours for breakthrough pain
Clindamycin 300mg
Fulfilled1 capsule 4× daily for 7 days
Prednisone 10mg
ExpiredTapering dose: 2 tablets × 3 days, 1 tablet × 3 days, ½ tablet × 3 days
Lidocaine Viscous 2%
Fulfilled15mL swish and spit 3× daily before meals
Doxycycline 100mg
Fulfilled1 capsule 2× daily for 14 days
Clinical Notes
SOAP notes, progress updates & AI-assisted documentationPatient states compliance is good, wearing aligners 21-22 hours/day. Mild discomfort with new tray for first 2 days, now resolved. No speech issues.
Aligners seat fully. Attachments intact on teeth #6, #7, #10, #11, #22, #23, #27. No debonds. ClinCheck comparison shows tracking well within expected range. IPR performed between #24-25 per plan (0.2mm).
Treatment progressing on schedule. Excellent patient compliance. Tooth movements tracking with ClinCheck prediction. No adverse events.
Dispense trays 9-11. Continue 14-day changes. Next IPR at tray 15 visit. Reinforce hygiene — slight plaque accumulation noted lingual of lower anteriors. Schedule next check in 4 weeks.
Treatment is on track. AI analysis of intraoral photos suggests slight tracking lag (<0.3mm) on tooth #10 rotation. No intervention needed at this stage. Recommend photo documentation at next visit for comparison.
35-year-old male, new to area. Chief complaint: "I want to fix my smile." Reports dissatisfaction with spacing between upper anterior teeth. No pain. Last dental visit 3 years ago. Medical history: seasonal allergies, no medications.
Full-mouth series taken. Comprehensive periodontal charting completed. Class I molar relationship bilaterally. Diastema 2.5mm between #8-9. Mild gingivitis noted on posteriors. Caries risk assessment: moderate. Oral cancer screening: negative.
Generalized mild chronic gingivitis. Diastema closure indicated for teeth #8-9. Caries risk moderate — recommend increased fluoride exposure. No urgent treatment needed.
Phase 1: Prophy, OHI, address gingivitis. Phase 2: Orthodontic consult for diastema closure (clear aligners vs traditional brackets). Phase 3: Restorative as needed after ortho. Discussed treatment sequence with patient. Patient elected to proceed with Phase 1.
Patient to schedule prophy. Will present ortho options at next visit.
Patient presents with spontaneous dull ache on lower right for 5 days. Pain wakes patient at night. Ibuprofen provides partial relief. No swelling. History: deep composite restoration placed on tooth #30 two years ago.
Tooth #30: large composite restoration with marginal staining. Percussion: tender. Palpation: WNL. Cold test: no response on #30 (adjacent #29, #31 respond normally within 3 sec). EPT: no response at 80/80. PA radiograph: periapical radiolucency ~4mm at apex of mesial root. No root fracture visible.
Necrotic pulp tooth #30 with symptomatic apical periodontitis. Non-restorable via conventional RCT due to curvature of mesial root. Endodontic referral indicated.
Referred to Dr. Endodontics Associates for evaluation and RCT. Prescribed Amoxicillin 500mg TID x 7 days for infection control. Patient advised to call if swelling develops. Follow-up after endo completion for permanent restoration.
High confidence recommendation for endodontic referral. CBCT imaging may be beneficial for treatment planning given mesial root curvature. Consider crown lengthening if insufficient ferrule after RCT. Coordinate with referring endodontist for integrated treatment timeline.
Good call on the referral. Mesial curvature is tricky — glad we are sending this out.
Agreed. Will follow up with endo office next week.
No comments yet. Be the first!